Enterohepatic circulation refers to the circulation of biliary acids, bilirubin, drugs or other substances from the liver to the bile, followed by entry into the small intestine, absorption by the enterocyte and transport back to the liver. Enterohepatic circulation is an especially important concept in the field of toxicology as many lipophilicxenobiotics undergo this process causing repeated liver damage.
Enterohepatic circulation allows for recycling of metabolized and non-metabolized compounds, and is of critical importance in toxicologic processes involving the gastrointestinal tract. This circulatory route is active when ingested compounds that are absorbed in the gastrointestinal tract enter the portal circulation, go to the liver, and then return to the gastrointestinal tract via biliary excretion. The enterohepatic circulatory pathway can also be utilized by dermally absorbed or inhaled materials that are excreted in the bile.
A compound leaves the enterohepatic circulation if it passes in the feces before being reabsorbed, or into the urine before being cleared by the liver. The ultimate destiny of a compound is dependent on its chemical composition and the species of animal exposed to the compound. The importance of species differences is best illustrated by the non-steroidal anti-inflammatory drug (NSAID) indomethacin, which undergoes enterohepatic circulation; it is excreted in the feces of dogs but in the urine of rats. The duration of enterohepatic circulation is most extensive for this drug in dogs and rats, and least extensive in rabbits and humans. This observation impacts resulting species-specific variability in toxicologic response of the GI tract to NSAIDs, with dogs being less tolerant of NSAID administration when compared to rats, rabbits, or humans.
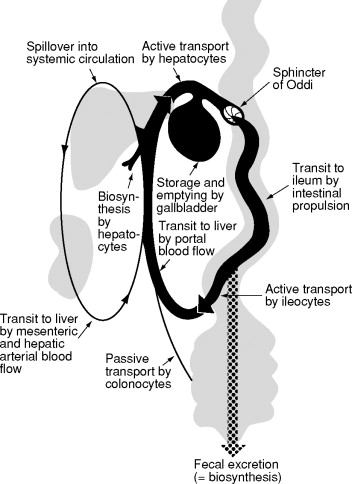
Figure 1. Schematic representation of the enterohepatic circulation of bile acids: see text for details. Reproduced from Hofmann AF (1992) Bile acids in liver and biliary disease. In: Millward-Sadler GH, Wright R, and Arthur MJP (eds) Wright’s Liver and Biliary Disease, 3rd edn, pp. 289–316. London, UK
Bile acid molecules are unique in that they are restricted to the enterohepatic circulation (Figure 1). They are secreted in bile as glycine and taurine conjugates, and are mainly absorbed by active transport in the distal ileum. Many other endogenous and exogenous compounds undergo some degree of enterohepatic circulation, but this usually represents a minor component of their tissue distribution. By contrast with bile acids, these substances are excreted in bile as glucuronate or sulfate conjugates, and deconjugation by colonic bacteria is essential for these molecules to reenter the enterohepatic circulation by passive colonic absorption following biliary excretion.
Hepatocytesmetabolizecholesterol to cholic acid and chenodeoxycholic acid. These lipid–solublebile acids are conjugated (reversibly attached) mainly to glycine or taurine molecules to form watersoluble primary conjugated bile acids, sometimes called “bile salts”. These bile acids travel to the gall bladder during the interdigestive phase for storage and to the descending part of the duodenum via the common bile duct through the major duodenal papilla during digestion. 95% of the bile acids which are delivered to the duodenum will be recycled by the enterohepatic circulation.
Due to the pH of the small intestine, most of the bile acids are ionized and mostly occur as their sodium salts which are then called “primary conjugated bile salts.” In the lower small intestine and colon, bacteria dehydroxylate some of the primary bile salts to form secondary conjugated bile salts (which are still water-soluble). Along the proximal and distal ileum, these conjugated primary bile salts are reabsorbed actively into hepatic portal circulation. Bacteria deconjugate some of the primary and secondary conjugated bile salts back to lipid-soluble bile acids, which are passively absorbed into hepatic portal circulation. Finally, the conjugated bile acids which remained un-ionized conjugated bile acids are passively absorbed.
Venous blood from the ileum goes straight into the portal vein and then into the liver sinusoids. There, hepatocytes extract bile acids very efficiently, and little escapes the healthy liver into systemic circulation.
The net effect of enterohepatic recirculation is that each bile salt molecule is reused about 20 times, often multiple times during a single digestive phase.
Function
The presence of biliary acids in the intestines helps in absorption of fats and other substances.
Bilirubin is conjugated with glucuronic acid in the liver by the enzyme glucuronyltransferase, making it soluble in water. Much of it goes into the bile and thus out into the small intestine. Although 20% of the secreted bilirubinoid bile is reabsorbed by the small intestine, conjugated bilirubin is not reabsorbed in small intestine.
All conjugated bilirubin in the large intestine is metabolised by colonic bacteria to urobilinogen, which is then further oxidized to urobilin and stercobilin. Urobilin, stercobilin and their degradation products give feces its brown color.
Kuntz, Erwin (2008). Hepatology: Textbook and Atlas. Germany: Springer. p. 38. ISBN978-3-540-76838-8.
However, just like bile, some of the urobilinogen reabsorbed is resecreted in the bile which is also part of enterohepatic circulation. The rest of the reabsorbed urobilinogen is excreted in the urine where it is converted to an oxidized form, urobilin, which gives urine its characteristic yellow color.
Drugs
Wikipedia lists the following drugs on the enterohepatic circulation page: chloramphenicol, aspirin, paracetamol, diazepam, lorazepam, morphine, metronidazole.
A number of drugs are secreted by the liver into bile, and are therefore capable of undergoing enterohepatic recycling. These include antibiotics, NSAIDS, hormones, opioids, digoxin, and warfarin.
Enterohepatic circulation of drugs is one of the pathogenetic factors in NSAID-induced intestinal epithelial damage.
NSAID-induced intestinal epithelial damage is due to direct effects after oral administration, recurrent local effects are due to enterohepatic recirculation of the drug, and systemic effects occur after absorption (Lanas and Sopena, 2009). Enterohepatic circulation refers to the phenomenon that drugs excreted into the intestine through bile are reabsorbed in the intestine and return to the liver through the portal vein (Gao et al., 2014). Bile duct ligation attenuated high dose indomethacin-induced intestinal perforation and death (Brodie et al., 1970a). Somasundaram et al. observed alterations in mitochondrial integrity of intestinal epithelial cells in indomethacin-treated rats, and bile duct ligation could prevent this early alteration (Somasundaram et al., 1997). In rats, four different NSAIDs were used to reveal a close relationship between the degree of enteropathy and the amount of drug secreted in the bile (Beck et al., 1990). All these experiments show that the enterohepatic circulation of drugs is one of the pathogenetic factors. Local effects of drugs are more important than systemic effects in the ulcerogenic effects of NSAIDs.
Mingyu Zhang, et. al., NSAID-Associated Small Intestinal Injury: An Overview From Animal Model Development to Pathogenesis, Treatment, and Prevention, Front. Pharmacol., 09 February 2022 Sec. Gastrointestinal and Hepatic Pharmacology Volume 13 – 2022 | https://doi.org/10.3389/fphar.2022.818877
The same article, definitely worth a read, says “Paracetamol leads to intestinal damage by inducing a process of apoptotic cell death of LGR5+ stem cells in the intestinal crypts, and the intestinal barrier function of paracetamol-treated mice is affected for a long time (Chopyk et al., 2019). Paracetamol administration leads to increased intestinal permeability as well as CCL7 upregulation, which promotes drug-induced liver injury (Niu et al., 2020).”
Mingyu Zhang, et. al., NSAID-Associated Small Intestinal Injury: An Overview From Animal Model Development to Pathogenesis, Treatment, and Prevention, Front. Pharmacol., 09 February 2022 Sec. Gastrointestinal and Hepatic Pharmacology Volume 13 – 2022 | https://doi.org/10.3389/fphar.2022.818877
Not only drugs but endogenous substrates like bilirubin, steroidal hormones and thyroxine utilize this pathway.
Enterohepatic circulation of drugs describes the process by which drugs are conjugated to glucuronic acid in the liver, excreted into bile, metabolized back into the free drug by intestinal bacteria, and the drug is then reabsorbed into plasma. For many drugs that undergo this process, lower doses of drugs can be therapeutically effective because elimination is reduced by the ‘recycling’ of the drug. But for a small number of drugs that are very toxic to the intestine (e.g. irinotecan), these molecules which would not otherwise be very toxic can become so because of this process, and therefore inhibition of this step can be protective. For the majority of drugs which undergo enterohepatic circulation that are not toxic to the intestine, inhibition of this process leads to a reduction of the levels of drug and reduced therapeutic effect. For example, antibiotics that kill gut bacteria often reduce enterohepatic drug circulation and this requires a temporary increase of the drug’s dose until the antibiotic use is discontinued and the gut repopulates with bacteria. This effect of antibiotics on enterohepatic circulation of other drugs is one of several types of drug interactions.
Pharmacokinetic Models of enterohepatic circulation
Pharmacokinetic models of the enterohepatic circulation process has been summarized in a recent article.
Mingyu Zhang, et. al., NSAID-Associated Small Intestinal Injury: An Overview From Animal Model Development to Pathogenesis, Treatment, and Prevention, Front. Pharmacol., 09 February 2022 Sec. Gastrointestinal and Hepatic Pharmacology Volume 13 – 2022 | https://doi.org/10.3389/fphar.2022.818877

{kind=link}
Leave a Reply